
More Information
Submitted: 31 August 2020 | Approved: 02 October 2020 | Published: 05 October 2020
How to cite this article: Ademe S, Mohammed M, Edmealem A. Knowledge and attitude of workers towards HIV post-exposure prophylaxis and exposure of staffs to sharp injuries in Dessie Referral Hospital: 2020; A cross sectional study. Clin J Nurs Care Pract. 2020; 4: 032-038.
DOI: 10.29328/journal.cjncp.1001025
Copyright License: © 2020 Ademe S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Knowledge; Hcws; Needle prick injury; Transmission; PEP (Post Exposure Prophylaxis)
Abbreviations: AIDS: Acquired Immune Deficiency Syndrome; ART: Antiretroviral Therapies; CDC: Communicable Diseases Control; HBV: Hepatitis B Virus; HCV: Hepatitis C Virus; HCWs: Health Care Workers; HIV: Human Immune Deficiency Virus; PPEs: Personal Protective Equipment’s; PEP: Post-Exposure Prophylaxis; US: United States, VCT: Voluntary Counselling and Testing

Knowledge and attitude of workers towards HIV post-exposure prophylaxis and exposure of staffs to sharp injuries in Dessie Referral Hospital: 2020; A cross sectional study
Sewunet Ademe1*, Mekia Mohammed2 and Afework Edmealem2
1Department of Nursing, Wollo University, Ethiopia
2Department of nursing, Tropical College of Medicine, Ethiopia
*Address for Correspondence: Sewunet Ademe, Department of Nursing, Wollo University, Ethiopia, Tel: +251918126233; Email: [email protected]
Background: Post exposure chemoprophylaxis can prevent human immunodeficiency virus (HIV) infection in risk healthcare workers; however routine adoptions of these practices by the workers have been limited.
Objective: To assess knowledge and attitude of health workers on HIV post-exposure prophylaxis and exposure to sharp injuries in Dessie referral hospital.
Methods: Across-sectional study was conducted on 422 health care workers of Dessie referral Hospital. The study subjects were selected by proportional allocation of each sample in its respective department/ward. Simple random sampling method was used to select study participants. The data was cleaned coded and analyzed by using statistical package for social sciences (SPSS) version 23. Finally the result was presented by graphs, pie chart and statements.
Results: A total of 422 study subjects were participated in the study. Among 422 participants 72.5% had good knowledge of post exposure prophylaxis for HIV and the rest 27.5% had poor knowledge of post exposure prophylaxis for HIV. Among 422 study participants 75.2% had positive attitude towards PEP.
283(67.1%) of them had exposure to sharp injuries.
Conclusion: Generally most of health care workers had good knowledge about post exposure prophylaxis against HIV/AIDS. This study had shown that a significant number of individuals had a negative attitude with regard to post exposure prophylaxis. Therefore, formal training that aims to improve attitudes and support to improve PEP implementation and completion are needed.
Each day thousands of healthcare workers (HCWs) around the world suffer accidental occupational exposures to blood borne pathogens. The WHO /International Labour Organization recommended the use of HIV post exposure prophylaxis (PEP) for prevention of HIV infection resulting from accidental injuries at work place [1,2].
Health care workers who have occupational exposure to blood are at increased risk for acquiring bloodborne infections. The level of risk depends on the number of patients with that infection in the health care facility and the precautions the health care workers observe while dealing these patients. The risk of HIV transmission is -0.3% after skin puncture. There have been rare reports of HIV transmission through exposure to mucous membrane (eyes, nose or mouth) or abraded (broken) skin, and the risk is estimated to be – 0.09 % [3,4].
Since the early 1990s, in many countries antiretroviral medicines have been prescribed for post-exposure prophylaxis (PEP) following occupational exposure to the human immune deficiency virus (HIV). PEP is a medical response to prevent transmission of HIV after potential exposure PEP is only effective if taken within 72 hours of the assault. In addition to a 28-day course of medicine to prevent HIV infection, people are given first aid care, counselling and follow-up visits [5-7].
Health care workers practicing in poor countries like Ethiopia are more exposed to HIV following occupational exposure and less likely to use PEP than those working in developed countries and well equipped facilities [8].
The World Health Organization estimates that 3 million percutaneous occupational exposures to blood or other body fluids occur in health care settings. CDC estimates 380,000 needle stick injuries in US hospital yearly. Ninety present of occupational exposure across the world occurred in developing countries [8]. Health providers are at risk of developing infections in their work place. The increasing prevalence of HIV increase the risk that health care workers will be exposed to blood from patients infected with HIV, especially when blood and body fluid precautions are not followed for all patients. Ethiopia is one of the hardest hit countries by HIV/AIDS epidemic with the national HIV prevalence of 1.4% in adults [9,10]. Practices, and re-duce anxiety, and/or increase staff retention and productivity. However literatures evidenced that there is an information gap in the health care setups. Therefore, the aim of this study was to assess knowledge attitude and practice of PEP in Dessie referral hospital [11]. On HIV post exposure prophylaxis few studies have been conducted, mainly focusing on injection safety; assessment of infection prevention practices in health care facilities and is a poorly researched area in Ethiopia.
This research may give some important information on the risk of transmission of blood borne pathogens like HIV, HCV and HBV.
This research paper may provide some important information for health program managers, researchers and other health professionals about the extent of sharp injuries towards exposure to HIV. Though this information is very important for the future for planning and implementation of effective strategies for health workers, patients and the community to minimize the potential risk of transmission of blood borne pathogens through considering health workers knowledge and attitude towards PEP.
General objective
To assess knowledge, attitude and exposure to sharp injuries of health workers on HIV post-exposure prophylaxis in Dessie referral hospital.
Specific objectives
• To assess knowledge of health care workers on HIV post-exposure prophylaxis in DRH from May to July.
• To assess attitude of health care workers on HIV post-exposure prophylaxis in DRH from May to July.
• To assess exposure to sharp injuries of health care workers on HIV post-exposure prophylaxis in DRH from May to July.
Study area and period
This study was conducted in Amhara region, South Wollo Zone, Dessie Referral Hospital. At North East Ethiopia at 401 km away from Addis Ababa, capital city of Ethiopia and 480 km from Bahirdar a capital city of ARS. It placed an Altitude of 8100 ft (2470 m). This study was conducted from May (2020) – July (2020).
Study design: Institutional based cross - sectional study design was conducted.
Source Population: All Health care workers of Dessie referral hospital
Study population: The study population was health professionals who were currently working in DRH directly involved in the care of patients (physicians, health officers, nurses, mid wives, and) in DRH in the data collection period.
Inclusion criteria: All health workers in Dessie Referral Hospital.
Exclusion criteria: Staffs that were in annual, material and study leave in Dessie Referral Hospital.
Sample Size determination: The sample size was calculated by using single population proportion formula.
where
• n = minimum sample size
• P = the proportion of the study 50%
• d = Margin of error i.e. =0.05
= Standard deviation at 95% = 1.96 (confidence level)
Taking to consideration the non-response rate of 10% of the total sample size of the study participants will be 422.
Sampling technique: Simple random sampling technique was used
Dependent variable
• Knowledge about HIV post-exposure prophylaxis
• Attitude about HIV post Exposure prophylaxis
• Exposure to sharp injuries
Independent variables
• Age
• Sex
• Religion
• Occupation
• Procedure done
• Educational background…etc
• Working environment
Data collection procedures
The data was collected by our group member using a self-administered questionnaire was given to the health care providers. The data collectors explained the objective of the study for the participants before they let them fill the questionnaire. Further, the data collectors mentioned as they clarified any ambiguous and unclear questions when necessary.
Data collection instrument
Data was collected by using a structured questionnaire. The questionnaire was prepared in English since the study participants were able to understand English language.
Data collectors` selection and training
To maintain the quality of the data, training was given for four data collectors for three days by the investigators about the confidentiality of the information and method of data collection.
Data collection method
Data collection was conducted using a structured self-administered questionnaire. Before the actual data collection began, pretest was done. After data collection was completed, each questioner was checked for completeness, missing values and unrelated responses.
Data quality management
To ensure the quality the data collection process was supervised, properly designing the questionnaire; proper training of the coordinators and supervisor about the data collection procedures.
Data processing, analysis, interpretation and presentation
After data collection, each questionnaire was checked visually for completeness and coding at the right margin of the questionnaire. The collected data was cleared and analysed by using SPSS version 23.
Finally the result was presented by graphs, pie chart and statements.
Ethical consideration
Data collection was started after the study was approved by the Institutional Ethics Review Committee of Wollo University then ethical clearance was taken from college of medicine and health sciences to get secured a permission letter from Dessie referral hospital administrators. Confidentiality of the records have maintained throughout the study period. Reports were not including names and identifiers of study participants.
Operational definitions
Good knowledge- those respondents who are able score > 70% of total knowledge questions
Poor knowledge - those respondents who are able to score < 70% of total knowledge questions.
Positive Attitude – those respondents who are able score > 70% of total attitude questions towards the infection prevention practice.
Negative attitude - is those respondents who are able to score < 70% of total attitude questions.
Good Practice – those respondents practicing at least > 70% of the practice questions in proper way.
Poor practice – those respondents who able to practicing at least < 70% of the practice questions in proper way.
Socio demographic characteristics of respondents
A total of 422 HCWs were involved, of which 177(41.9%) were females and 245(58.1%) were males. Most of the respondents, 328(77.7%) were in the age group of 26 to 30 years with a mean age of 26.2 years. The majority of the participants were nurses (93.1%), of whom 72% had less than five year of experience (Table 1).
| Table 1: Socio demographic characteristics of HCWs at Dessie referral Hospital in Dessie city administration, June, 2020 (n = 422). | ||
| Variable | Categories | N(%) |
| Age | 20-25 26-30 31-35 36-45 |
41(9.7%) 287(68.0%) 79(18.7%) 15(3.6%) |
| Sex | Female Male |
177(41.9%) 245(58.1%) |
| Working Area(Unit) | Adult OPD and Medical ward Pedi OPD and Ward Gyni and Obse Emergences Surgical ward and Others |
85(20.1%) 85(20.1%) 84(19.9%) 84(19.9) 84(19.9%) |
| Ethinic Group | Amhara | 335(79.4%) |
| Tigrie Oromo Afar |
77(18.2%) 3(.7%) 7(1.7%) |
|
| Marital Status | Single Married Divorced Widowed |
196(46.4%) 206(48.8%) 17(4.0%) 3(.7%) |
| Educational Level | Diploma Degree Masters PHD Specialist |
105(24.9%) 288(68.2%) 24(5.7%) 4(0.9%) 1(.2%) |
| Service Year | Less than two year Three up to five year Six up to ten year More than ten year |
95(22.5%) 209(49.5%) 97(23.0%) 21(5.0%) |
Knowledge Level of the HCWs about PEP for HIV
In the current study, 306(72.5%) of the participants had good knowledge about PEP for HIV. 381(90.3%) respondents heard about PEP for HIV infection, The majority of the study participants knew the preferred time to initiate PEP 265(62.8%). 297(70.4%) individuals knew PEP medications taken for 28 days. 345(81.8%) individuals knew follow up is important for PEP, 116(27.5%) study participants had poor knowledge about PEP (Table 2).
Table 2: Knowledge about PEP for HIV among healthcare workers in DRH, in Dessie city administration, June, 2020 (n = 422). |
||
| Knowledge questions | Responses | Frequency (%) |
| Heard about PEP | Yes no |
381(90.3%) 41(9.7%) |
| Know PEP is available at your hospital | Yes No |
337(79.9%) |
| 94(22.3%) | ||
| Accessible to get PEP at your hospital |
Yes No |
328(77.7%) 94(22.3%) |
| To be effective PEP must begin within 72 hours |
Yes No |
265(62.8%) 157(37.2%) |
| PEP medication should be taken for sharp injuries | Yes No |
297(70.4%) 125(29.6%) |
| Follow up is important after PEP was taken | Yes No |
345(81.8%) 77(18.2%) |
| Should take PEP during non-blood body fluids contacts | Yes No |
280(66.4%) 142(33.6%) |
| knowing transmission of disease during exposure to body fluids | Yes No |
330(78.2%) 92(21.8%) |
| Need PEP for superficial injury | Yes No |
304(72.0%) |
| 118(28.0%) | ||
| Knowing where to go to take PEP if you have exposure | Yes No |
327(77.5%) 75(22.5) |
Knowledge questions Responses Frequency (%).
Attitude of the HCWs about PEP for HIV
Greater than half, 317 (75.2%), of the study participants had a positive attitude about PEP. The majority of the respondents, 375 (89%) and 360(80.6%), agreed on the benefit of PEP and availability of PEP guidelines in their work place, respectively. The majority of individuals (80.6%) believed that PEP can reduce the likelihood of acquiring HIV after being exposed. However, only 21 (78.9%) of the participants believed that PEP should be indicated for any type of sharp object injuries. 252 (71.3%) individuals had no trust in PEP effectiveness. Whereas 104.6(24.8%) respondents had poor knowledge about PEP (Table 3) (Figures 1,2).
| Table 3: Attitude of HCWs about PEP at Dessie referral hospital, in Dessie city administration, June, 2020 (n = 422). | |||||
| Attitude questions | Strongly agree | Agree | Don’t know | Disagree | Strongly Disagree |
| PEP should be compulsory for CWs |
196(46.4%) | 179(42.6%) | 34(8.1%) | 5(1.2%) | 7(1.7%) |
| PEP is 100% effective | 107(25.4%) | 233(55.2%) | 38(9.0%) | 30(7.1%) | 14(3.3%) |
| PEP must available at any time and place |
170(40.3%) | 190(45.0%) | 29(6.9%) | 32(7.6%) | 1(0.2%) |
| scared of taking PEP | 147(34.8%) | 152(36.0%) | 61(14.5%) | 47(11.1%) | 15(3.6%) |
| I do not trust PEP | 133(31.5%) | 168(39.8%) | 44(10.4%) | 62(14.7%) | 15(3.6%) |
| PEP is against my religion |
104(24.6%) | 149(35.3%) | 73(17.3%) | 67(15.9%) | 29(6.9%) |
| If sustain injury you should take PEP |
129(30.6%) | 204(48.3%) | 50(11.8%) | 31(7.3%) | 8(1.9%) |
| Exposure non-blood fluids is also risky |
130(30.8%) | 186(44.1%) | 58(13.7%) | 35(8.3%) | 13(3.1%) |
| Washing with saline is not adequate to |
85(20.1%) | 202(47.9%) | 58(13.7%) | 68(16.1%) | 9(2.1%) |
| PEP must affordable | 134(31.8%) | 175(41.5%) | 58(13.7%) | 41(9.7%) | 14(3.3%) |
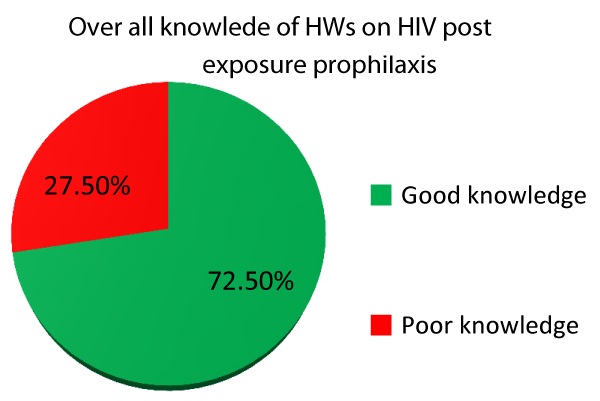
Figure 1: Overall knowledge of HCWs on PEP in DRH in Dessie referral hospital in Dessie city administration, June, 2020 (n = 422).
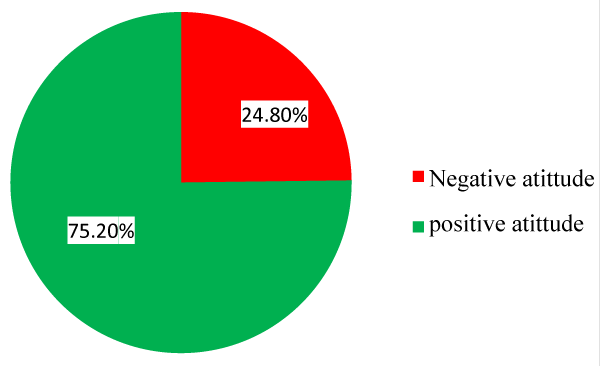
Figure 2: Overall attitudes of HCWs on HIV PEP in Dessie referral hospital in Dessie city administration, June, 2020 (n = 422).
Exposure of HCWs for sharp injuries in DRH
Of the 422 (100%) study participant 283(67.1%) individuals had exposures for HIV risky conditions. Among the individuals who expose to HIV risky condition 163(38.6%) are due to slight skin penetration, 124(29.4%) were exposed due to deep injury, 42(10.0%) individuals had exposed due to exposure to blood and body fluid in the skin, 104(24.7%) individuals exposed by blood and body fluids in mucous membrane. And 67(15.9%) individuals exposed by splash to the eye (Table 4).
| Table 4: Practice of PEP for HIV among HCW in Dessie referral hospital in Dessie city administration, June, 2020 (n = 422). | ||
| Practice | Response | Frequency (%) |
| Needle sticks injury since the past one year | Yes | 283(67.1%) |
| No | 139(32.9%) | |
| what type of injury you sustained | Deep injury | 124(29.4%) |
| Slight skin penetration | 163(38.6%) | |
| Superficial injury | 42(10.0%) | |
| Others, specify | 93(22.0%) | |
| How many needle stick injuries did you sustain in the last in the last one year |
Never | 201(47.6%) |
| I don’t remember | 45(10.6%) | |
| Once only | 124(29.4%) | |
| 2-5 Times | 34(8.1%) | |
| More than 5 times | 18(4.3%) | |
| How did you sustain that injury | During recapping | 187(44.3%) |
| Others | 58(13.8%) | |
| By sudden movement of a patient during injection | 142(33.6%) | |
| During sharp collection | 35(8.3%) | |
| Have you had any injury by sharps (scissors, blade) since last year | Yes | 228(54.4%) |
| No | 129(30.6%) | |
| Type of injury you sustained | Deep injury | 127(30.1%) |
| Others | 109(25.8%) | |
| Slight skin penetration | 24(5.7%) | |
| Superficial | 21(5.9%) | |
| Have you ever been exposed to any blood and body fluids | Yes | 277(78.5%) |
| No | 76(21.5%) | |
| What type of exposure (blood and body fluids) did you have |
Exposure of blood and body fluids to skin | 223(53.0%) |
| If u sustain injury what was u do | Exposure of blood and body Fluids to mucous membranes | 104(24.7%) |
What type of exposure (blood and body fluids) did you have to mucous membranes.
In this study the KAP of HCWs towards PEP in Dessie referral hospital were assessed. This study had shown that high proportion of health care workers were knowledgeable. Three hundred six (72.5%) had good knowledge of PEP for HIV and the remaining 27.5 % of respondents had poor knowledge. This is lower than similar studies from Gonder University hospital (36.9% of health workers had poor knowledge) [14], Nigeria (7% - 29%), and Cameroonian health district (28.3%)[15]. This difference might be due to the advantage of having special trainings of health care workers in DRH and year of study conducted. Greater than 75% of study participants had completed their bachelor degree or medical doctor; this higher level of education may explain the higher knowledge demonstrated by our participants.
In this study, greater than 90.3% participants had heard about PEP for HIV. This level of awareness among these study participants was higher than similar study in Hawassa University Hospital (67.1%) [21], and lower than tertiary Hospital of Nigeria (97%) [19] And in line with Gonder university hospital (92.8%) [14]. This difference might be they might had more trainings as compared with DRH’s health care worker, sample size and year of study conducted.
Regarding timing and duration of PEP for HIV, 265(62.8%) of the total respondents stated that PEP should be taken within 72 hour and 297(70.4%) of them knew the correct duration of PEP against HIV/AIDS (28 days). A study conducted among Interns of a Medical College in West Bengal, India, indicated only 60.5% stated PEP should be started within 72 hours of exposure and only 46.9% conveyed appropriate duration of PEP (28 days) [25]. The difference might be due to differences in the work experience as greater than 77.3% of this participants had professional experience of greater than three years. In addition, this result showed that greater awareness on timing of PEP among our HCWs than other studies from Uganda (22.3%) [26], Mumbai (59%) [27], and Gondar (50.8) [14]. This difference might be due to sample size, study design, year of study conducted and might be due to health system of countries.
The majority 75.2% of study participants had a positive attitude towards PEP. 89% of study participant were agreed on the importance of PEP for health care workers. A study conducted at the Gondar University Hospital indicated that 98.5% agreed on the importance of PEP for HIV [14], which is greater than this study (89%). The difference might be due to fear of adverse effect of ART drug and 69.5% agreed that PEP guidelines should be available in the hospital which is lower than our study (80.6%). This was might be aware of ever thing in their work place and taking PEP. Of the 422 study subjects, 283(67.1%) of the participants have been exposed to HIV risky conditions. This finding is lower than the result found in the research done in the Jimma zone on government HCWs (68.50%) [2], this difference might be due to strict following precautions and wearing PPE. And higher than Gondar University Hospital (33.8%) [14], this might be due to high level of precaution and wearing of proper personnel protective equipment’s in this study area compared to these study participants. Higher exposure of our study participants to risky conditions might be due to inadequate knowledge in our study group. However, the number of HCWs that have ever been exposed to HIV risky conditions in our study is not considered low. However, a study conducted in Gujarat, India [29], showed that their 90% respondents exposed to HIV risky condition on practice in this regard higher than this study participants (67.1%) were exposed. This fact alerts that the practice of PEP for HIV in this study area needs improvement. Reasons for the observed difference of findings between different research results might be due to the difference in the level of awareness among the different population, economic difference of the study population, and time difference of the studies.
Limitations of study
The statistical analysis was descriptive and unable to determine association of independent variables with the outcome. The simple random sampling technique was also the major limitation of the present study may not have chance of representativeness.
Most of HCWs have good knowledge about PEP after occupational risk of HIV/AIDS exposure and had a positive attitude towards PEP for occupational risk of HIV infection. The findings of this study revealed the attitude and practice of HCWs towards PEP for HIV is adequate. A significant proportion of HCWs have had exposure for sharp injuries. This compounded by low PEP completion rates shows that the practice of PEP for HIV in this study area needs improvement.
Recommendation
✍ Regular education and training for HCWs in frequent intervals should be carried out.
✍ Hospital management should document the accidental exposure of HCWs to factor of HIV.
✍ The guideline for precaution measures and disseminate among HCWs should be prepared.
✍ Drugs for PEP should be made available in every hospital, and in cases treatment should be immediately initiated.
This article was sponsored by Tropical College of medicine Dessie campus. The authors would like to appreciate Dessie referral hospital staffs for their participants as well as officials who helped us in this research development.
Funding: Tropical College of medicine Dessie campus.
Availability of data and materials: Data are available by contacting the corresponding author.
Authors ‘contributions: SA contributed to designing the study and wrote the final report and manuscript, MM and AE collected the data analysed the data. All the authors read and approved the version for submission.
Ethics approval and consent to participate: Ethical approval was obtained from the Ethical Review Committee of Wollo University. Permission letter was received from Dessie referral hospital.
Consent for publication: All the participants consented to publish the study in this journal.
- World Health Organization (WHO). HIV /AIDS, post exposure prophylaxis. 2013.
- United Nation. Post-exposure prophylaxis (PEP) to prevent HIV infection. Guidelines on the use of treatment Starter Kits. 2008.
- www.unescobkk.org/fileadmin/user.upload HIV/AIDS /Documents/Workplace/pepe.pdf
- World Health Organization (WHO) International Labor Organization (ILO). Joint ILO/WHO guidelines on health services and HIV /AIDS. 2005.
- Kermode M. Unsafe Injections in Low-Income Country Health Settings: Need for Injection Safety to Prevent the Spread of Blood Borne Viruses. Health Promotion International. 2004; 19: 95-103. PubMed: https://pubmed.ncbi.nlm.nih.gov/14976177
- National Center for AIDS & STD controls (NCASC). National anti- retroviral therapy guidelines. 2009.
- United Nation. Post-exposure prophylaxis (PEP) to prevent HIV infection. Guidelines on the use of treatment Starter Kits. www.unescobkk.org/fileadmin/user_upload/ HIV/AIDS/Documents/Workplace/pepe.pdf
- Sharma A, Marfatia YS, Ghia R. post –exposure prophylaxis for HIV. Indian J Sexual Transmission Diseases AIDS. 2007; 28: 61-68.
- Wig N. HIV: awareness of management of occupational exposure in health care workers. Indian J Med Sci. 2003; 57: 192-198. PubMed: https://pubmed.ncbi.nlm.nih.gov/14514250/
- Amanuel G, Araya K. Occupational Exposure of Health Workers to Blood and Body Fluids. Ethiopian Public Health Association Oral Abstracts, 18th Annual Conference. 2007.
- Many Chen GX, Jenkins EL. Potential Work Related Exposures to Blood Borne Pathogens By Industry And Occupation In The United States Part II: A Telephone Interview Study. Am J Industrial Med. 2007; 50: 285-292.
- Sharma R, Rasania SK, Verma A, Singh S. Study of prevalence and response to needle stick injuries among health care workers in a tertiary care hospital in Delhi, India. Indian J Community Med. 2010; 35: 74-77. PubMed: https://pubmed.ncbi.nlm.nih.gov/20606925/
- Alenyo R, Fualal J, Jombw JJ. Knowledge, Attitude and Practices of Staffs towards Post-exposure Prophylaxis for HIV Infection at Mulago Hospital in Uganda. East Central African J Surg. 2009; 14: 99-102.
- Tetali S, Choudhury PL. Occupational exposure to sharps and splash: Risk among health care providers in three tertiary care hospitals in South India. Indian J Occup Environ Med. 2006; 10: 35-40.
- Endalew Gemechu Sendo, Addis Ababa University, College of Health Science, School of Nursing and Midwifery, Addis Ababa, Ethiopia, www.peertechz.com
prophylaxis guidelines against occupational exposure to HIV in Hospital Sungai Petani. Med JMalaysia. 2005; 60: 10-14. - WHO. AIDS epidemic update: December 2006. Geneva: UNAIDS/WHO.
- Chagani MM, Manji KP, Manji MP, Sheriff FG. Healthcare workers’ knowledge, attitudes, practices on post exposure prophylaxis for HIV in Dares Salaam. Tanzania Med J. 2011; 25: 33-38.
- Bandolier E. Occupational exposure to hospital employees in Italian hospitals over 5.5 years. 2003.
- Bosena T, Hailu C. Assessment of HIV Post Exposure Prophylaxis use Among Health Worker of Governmental Health Institutions in Jimma zone, Oromiya Region, Southwest. Ethiopia. Ethiop J Health Sci. 2010. 20: 55–64. PubMed: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3275901/
- Gupta A, Anand S, Sastry J, Krisagar A, Basavaraj A, et al. High risk for occupational exposure to HIV and utilization of post-exposure prophylaxis in a hospital in Pune, India. BMC Infectious Diseases. 2008; 8: 142. PubMed: https://pubmed.ncbi.nlm.nih.gov/18939992/
- Infection prevention and control (home page on the internet). 2007. http://www.jhpiego.org
- Pruss-Ustun A, Rapiti E, Hutin Y. Estimation of The Global Burden of Disease attributable to Contaminated Sharps Injuries among Health Care Workers. Ame J Industrial Med. 2005; 48: 482-490. PubMed: https://pubmed.ncbi.nlm.nih.gov/16299710/
- Jovic-Vranes A, Jankovic S, Vukovic D, et al. Risk Perception and Attitudes towards HIV in Serbian Health Care Workers. Occupational Medicine. 2006; 56: 275–278. PubMed: https://pubmed.ncbi.nlm.nih.gov/16627545/
- Moens G, Mylle G, Johannik. Experience of Health Care Workers Taking Post-Exposure Prophylaxis after Occupational HIV Exposures: Findings of the HIV Pos-Exposure Prophylaxis Registry. Infection Control Hospital Epidemiol. 2000; 21: 780-785.
- The prevalence of needle stick injuries in Medical, Dental, Nursing and Midwifery Students at the university Teaching Hospitals of Shiraz, Iran Mehardad Askarian, Leila melekmakan Medical Bulletin. 2006; 60: 227-232. PubMed: https://pubmed.ncbi.nlm.nih.gov/16790948/
- Jovic-Vranes A, Jankovic S, Vukovic D, et al. Risk Perception and Attitudes towards HIV in Serbian Health Care Workers. Occupational Med. 2006; 56: 275–278. PubMed: https://pubmed.ncbi.nlm.nih.gov/16627545/
- Gershon R. Facilitator Report: Blood Borne Pathogens Exposure among Health Care Workers. Am J Industrial Med. 1996; 29: 418-420.
- Julian G, Maggy T. Occupational Post Exposure Prophylaxis for HIV: Australia, 2005.
- Lee CH, Carter WA, Chiang WK, et al. Occupational Exposures to Blood among Emergency Medicine Residents. Acade Emerg Med. 1999; 6: 1036-A1043. PubMed: https://pubmed.ncbi.nlm.nih.gov/10530663/